展开查看详情
1 . Tool Detection and Operative Skill Assessment in
Surgical Videos Using Region-Based Convolutional
Neural Networks
Amy Jin, Serena Yeung, Jeffrey Jopling, Jonathan Krause, Dan Azagury,
Arnold Milstein, and Li Fei-Fei
Stanford University
Stanford, CA 94305
{ajin,serena,jkrause,feifeili}@cs.stanford.edu
{jjopling,dazagury,amilstein}@stanford.edu
Abstract
Five billion people in the world lack access to quality surgical care. Surgeon
skill varies dramatically, and many surgical patients suffer complications and
avoidable harm. Improving surgical training and feedback will help to reduce the
rate of complications—half of which have been shown to be preventable. To do
this, it is essential to assess operative skills, a process that is currently manual,
time consuming, subjective, and requires experts. In this work, we introduce an
approach to automatically assess surgeon performance by tracking and analyzing
tool movements in surgical videos, leveraging region-based convolutional neural
networks. In order to study this problem, we also introduce a new dataset, m2cai16-
tool-locations, which extends the m2cai16-tool dataset with spatial bounds of
tools. While previous methods have addressed tool presence detection, ours is
the first to not only detect presence but also spatially localize surgical tools in
real-world surgical videos. We show that our method both effectively detects the
spatial bounds of tools as well as significantly outperforms existing methods on
tool presence detection. We further demonstrate the ability of our method to assess
surgical quality through analysis of tool usage patterns, movement range, and
economy of motion.
1 Introduction
According to the World Health Organization, there is a global mortality rate of 0.5-5% for major
procedures, and up to 25% of surgical patients suffer complications [1]. Many of these complications
are caused by poor individual and team performance, for which inadequate training and feedback play
an important role [2, 3, 4]. These outcomes can be improved, as studies show that half of all adverse
surgical events are preventable. One major challenge to improving these outcomes is that surgeons
currently lack individualized, objective feedback on their surgical technique. Real time automated
surgical video analysis can provide a way to objectively and efficiently assess surgical skill.
In this work, we address this task of spatial tool detection, which to our knowledge has not been
previously studied. In order to study this, we introduce a new dataset, m2cai16-tool-locations, which
extends the m2cai16-tool dataset with spatial bounds of tools. We develop an approach leveraging
region-based convolutional neural networks (R-CNNs) to perform spatial detection of tools, and show
that our method is able to both effectively detect the spatial bounds of tools as well as significantly
outperform previous work on detecting tool presence. Finally, we demonstrate that our spatial
detections in these real-world surgical videos enables efficient assessment of surgical quality through
analysis of tool usage patterns, movement range, and economy of motion.
31st Conference on Neural Information Processing Systems (NIPS 2017), Long Beach, CA, USA.
�
2 .Figure 1: Top: the seven tools and their annotation counts in m2cai-16-tool-locations. Bottom: example frames
with their spatial tool annotations. Color of the bounding box corresponds to tool identity.
2 Related Work
Early work on surgical tool detection, categorization, and tracking include those based on radio
frequency identification (RFID) tags [5]; segmentation, contour processing and 3D modelling [6];
and the Viola-Jones detection framework [7]. Furthermore, deep learning approaches based on
convolutional neural networks have shown impressive performance on computer vision tasks [8],
and works including [9, 10, 11, 12] leverage deep learning architectures to achieve state-of-the-art
performance on surgical tool presence detection and phase recognition. Our work builds on these
directions, and uses region-based convolutional neural networks [13] to detect the spatial bounds of
tools and enable richer analysis of surgical quality.
3 Dataset
In order to study the task of spatial tool detection, a dataset containing annotations of spatial bounds
of tools is required. However, to the best of our knowledge, no such dataset currently exists for
real-world laparoscopic surgical videos. We therefore collect and introduce a new dataset, m2cai16-
tool-locations, which extends the m2cai16-tool dataset [14] with spatial annotations of tools.
m2cai-16-tool consists of 15 videos recorded at 25 fps of cholecystectomy procedures. The dataset
contains 23,000 frames labeled with binary annotations indicating presence or absence of seven
surgical tools: grasper, bipolar, hook, scissors, clip applier, irrigator, and specimen bag. In m2cai16-
tool-locations, we label 2532 of the frames, with the coordinates of spatial bounding boxes around
the tools. We use 50%, 30%, and 20% for training, validation, and test splits.
4 Approach
Our approach for spatial detection of surgical tools is based on Faster R-CNN [13], a region-based
convolutional neural network. The input is a video frame, and the output is the spatial coordinates
of bounding boxes around any of the seven surgical instruments in Fig. 1. This output allows us to
perform qualitative and quantitative analyses of tool movements, from tracking tool usage patterns to
evaluating motion economy.
The base network is a VGG-16 convolutional neural network [15], which extracts powerful visual
features. On top of this network is a region proposal network (RPN) that shares convolutional
features with object detection networks. For each input image, the RPN generates region proposals
likely to contain an object, and features are pooled over these regions before being passed to a final
classification and bounding box refinement network.
We pre-train the network on the ImageNet dataset [8], where a large amount of data is available to
learn general visual features, and then fine-tune the network on our m2cai16-tool-locations dataset,
where a smaller amount of data is labeled with the surgical tools of interest.
To train the RPN, we assign a binary objectness label to each anchor at each sliding window position
of the feature map. We also assign a positive label to anchors with an overlap greater than 0.8 with
the ground-truth box or if those do not exist, to an anchor or anchors with the highest Intersection
over Union (IoU), and a negative label to anchors with an IoU of less than 0.3.
We fine-tune the VGG-16 network to optimize model performance using stochastic gradient descent.
We modify the classification layer of the network to output softmax probabilities over the 7 tools.
2
�
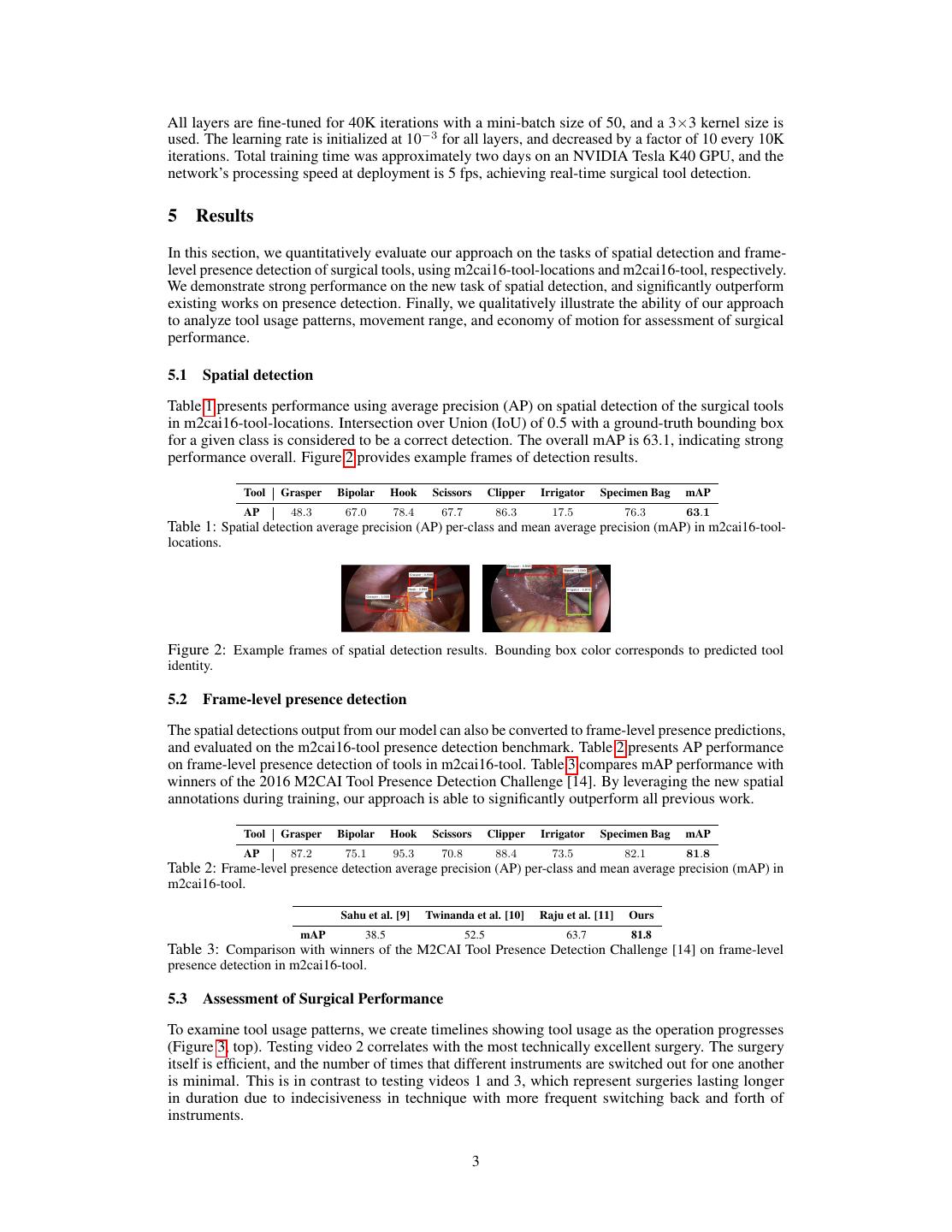
3 .All layers are fine-tuned for 40K iterations with a mini-batch size of 50, and a 3×3 kernel size is
used. The learning rate is initialized at 10−3 for all layers, and decreased by a factor of 10 every 10K
iterations. Total training time was approximately two days on an NVIDIA Tesla K40 GPU, and the
network’s processing speed at deployment is 5 fps, achieving real-time surgical tool detection.
5 Results
In this section, we quantitatively evaluate our approach on the tasks of spatial detection and frame-
level presence detection of surgical tools, using m2cai16-tool-locations and m2cai16-tool, respectively.
We demonstrate strong performance on the new task of spatial detection, and significantly outperform
existing works on presence detection. Finally, we qualitatively illustrate the ability of our approach
to analyze tool usage patterns, movement range, and economy of motion for assessment of surgical
performance.
5.1 Spatial detection
Table 1 presents performance using average precision (AP) on spatial detection of the surgical tools
in m2cai16-tool-locations. Intersection over Union (IoU) of 0.5 with a ground-truth bounding box
for a given class is considered to be a correct detection. The overall mAP is 63.1, indicating strong
performance overall. Figure 2 provides example frames of detection results.
Tool Grasper Bipolar Hook Scissors Clipper Irrigator Specimen Bag mAP
AP 48.3 67.0 78.4 67.7 86.3 17.5 76.3 63.1
Table 1: Spatial detection average precision (AP) per-class and mean average precision (mAP) in m2cai16-tool-
locations.
Figure 2: Example frames of spatial detection results. Bounding box color corresponds to predicted tool
identity.
5.2 Frame-level presence detection
The spatial detections output from our model can also be converted to frame-level presence predictions,
and evaluated on the m2cai16-tool presence detection benchmark. Table 2 presents AP performance
on frame-level presence detection of tools in m2cai16-tool. Table 3 compares mAP performance with
winners of the 2016 M2CAI Tool Presence Detection Challenge [14]. By leveraging the new spatial
annotations during training, our approach is able to significantly outperform all previous work.
Tool Grasper Bipolar Hook Scissors Clipper Irrigator Specimen Bag mAP
AP 87.2 75.1 95.3 70.8 88.4 73.5 82.1 81.8
Table 2: Frame-level presence detection average precision (AP) per-class and mean average precision (mAP) in
m2cai16-tool.
Sahu et al. [9] Twinanda et al. [10] Raju et al. [11] Ours
mAP 38.5 52.5 63.7 81.8
Table 3: Comparison with winners of the M2CAI Tool Presence Detection Challenge [14] on frame-level
presence detection in m2cai16-tool.
5.3 Assessment of Surgical Performance
To examine tool usage patterns, we create timelines showing tool usage as the operation progresses
(Figure 3, top). Testing video 2 correlates with the most technically excellent surgery. The surgery
itself is efficient, and the number of times that different instruments are switched out for one another
is minimal. This is in contrast to testing videos 1 and 3, which represent surgeries lasting longer
in duration due to indecisiveness in technique with more frequent switching back and forth of
instruments.
3
�
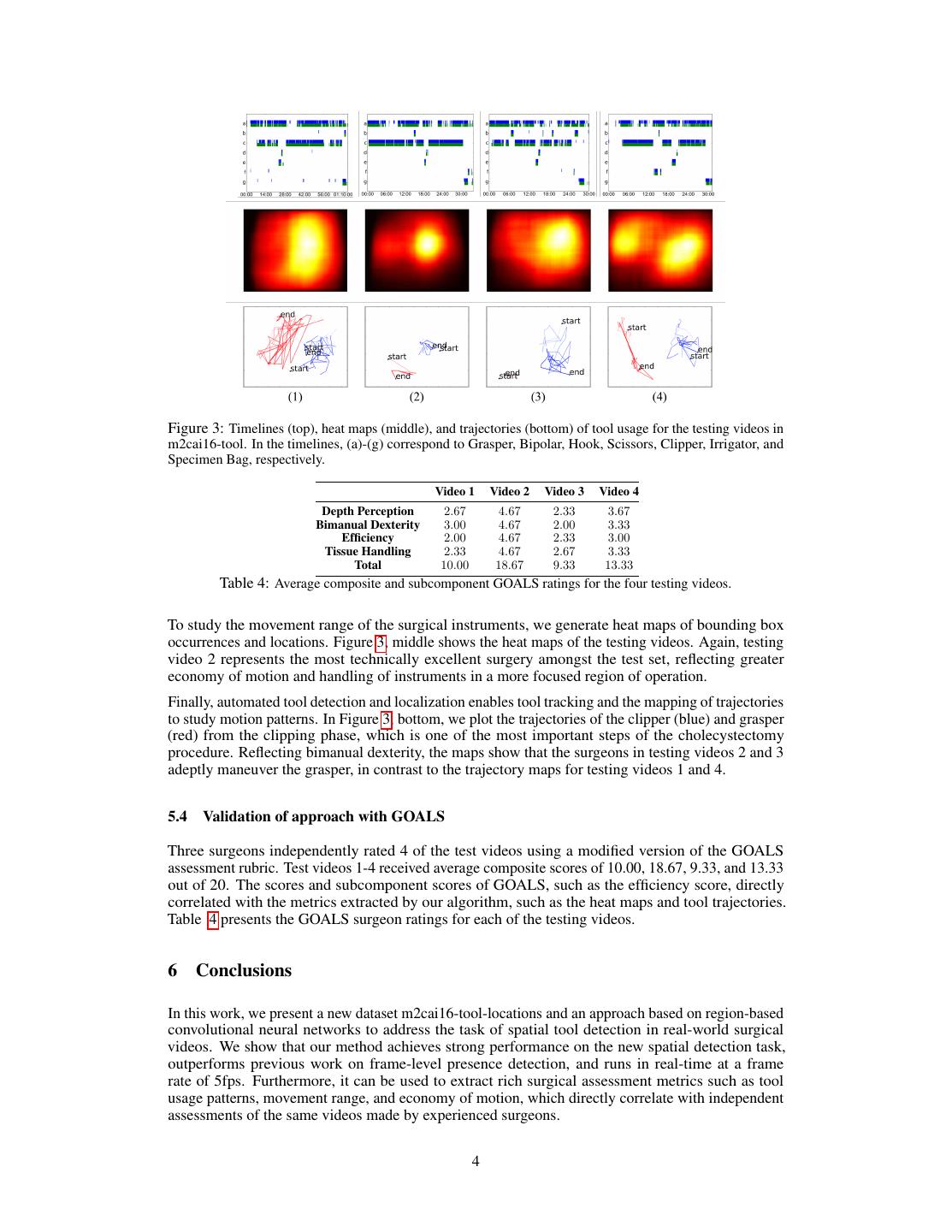
4 .Figure 3: Timelines (top), heat maps (middle), and trajectories (bottom) of tool usage for the testing videos in
m2cai16-tool. In the timelines, (a)-(g) correspond to Grasper, Bipolar, Hook, Scissors, Clipper, Irrigator, and
Specimen Bag, respectively.
Video 1 Video 2 Video 3 Video 4
Depth Perception 2.67 4.67 2.33 3.67
Bimanual Dexterity 3.00 4.67 2.00 3.33
Efficiency 2.00 4.67 2.33 3.00
Tissue Handling 2.33 4.67 2.67 3.33
Total 10.00 18.67 9.33 13.33
Table 4: Average composite and subcomponent GOALS ratings for the four testing videos.
To study the movement range of the surgical instruments, we generate heat maps of bounding box
occurrences and locations. Figure 3, middle shows the heat maps of the testing videos. Again, testing
video 2 represents the most technically excellent surgery amongst the test set, reflecting greater
economy of motion and handling of instruments in a more focused region of operation.
Finally, automated tool detection and localization enables tool tracking and the mapping of trajectories
to study motion patterns. In Figure 3, bottom, we plot the trajectories of the clipper (blue) and grasper
(red) from the clipping phase, which is one of the most important steps of the cholecystectomy
procedure. Reflecting bimanual dexterity, the maps show that the surgeons in testing videos 2 and 3
adeptly maneuver the grasper, in contrast to the trajectory maps for testing videos 1 and 4.
5.4 Validation of approach with GOALS
Three surgeons independently rated 4 of the test videos using a modified version of the GOALS
assessment rubric. Test videos 1-4 received average composite scores of 10.00, 18.67, 9.33, and 13.33
out of 20. The scores and subcomponent scores of GOALS, such as the efficiency score, directly
correlated with the metrics extracted by our algorithm, such as the heat maps and tool trajectories.
Table 4 presents the GOALS surgeon ratings for each of the testing videos.
6 Conclusions
In this work, we present a new dataset m2cai16-tool-locations and an approach based on region-based
convolutional neural networks to address the task of spatial tool detection in real-world surgical
videos. We show that our method achieves strong performance on the new spatial detection task,
outperforms previous work on frame-level presence detection, and runs in real-time at a frame
rate of 5fps. Furthermore, it can be used to extract rich surgical assessment metrics such as tool
usage patterns, movement range, and economy of motion, which directly correlate with independent
assessments of the same videos made by experienced surgeons.
4
�
5 .References
[1] T. Weiser, S. Regenbogen, K. Thompson, et al. An estimation of the global volume of surgery: a modelling
strategy based on available data. The Lancet, 372(9633):139–144, 2008.
[2] A. Gawande, E. Thomas, M. Zinner, and T. Brennan. The incidence and nature of surgical adverse events in
Colorado and Utah in 1992. Surgery, 126(1):66–75, 1999.
[3] M. Healey, S. Shackford, T. Osler, F. Rogers, and E. Burns. Complications in surgical patients. Archives of
Surgery, 137(5):611–618, 2002.
[4] A. Kable, R. Gibberd, and A. Spigelman. Adverse events in surgical patients in Australia. International
Journal for Quality in Health Care, 14(4):269–276, 2002.
[5] M. Kranzfelder, A. Schneider, A. Fiolka, et al. Real-time instrument detection in minimally invasive surgery
using radiofrequency identification technology. Journal of Surgical Research, 185(2):704–710, 2013.
[6] S. Speidel, J. Benzko, S. Krappe, et al. Automatic classification of minimally invasive instru- ments based
on endoscopic image sequences. In SPIE Medical Imaging, pages 72610A–72610A. International Society for
Optics and Photonics, 2009.
[7] F. Lalys, L. Riffaud, D. Bouget, and P. Jannin. A framework for the recognition of high-level surgical tasks
from video images for cataract surgeries. IEEE Transactions on Biomedical Engineering, 59(4):966–976, 2012.
[8] O. Russakovsky, J. Deng, H. Su, J. Krause, S. Satheesh, S. Ma, Z. Huang, A. Karpathy, A. Khosla, M.
Bernstein, et al. Imagenet large scale visual recognition challenge. International Journal of Computer Vision,
115(3):211–252, 2015.
[9] M. Sahu, A. Mukhopadhyay, A. Szengel, and S. Zachow. Tool and phase recognition using contextual CNN
features. 2016.
[10] A. Twinanda, D. Mutter, J. Marescaux, M. de Mathelin, and N. Padoy. Single-and multi- task architectures
for tool presence detection challenge at M2CAI 2016. arXiv preprint arXiv:1610.08851, 2016.
[11] A. Raju, S. Wang, and J. Huang. M2CAI surgical tool detection challenge report. 2016.
[12] A. Twinanda, S. Shehata, D. Mutter, J. Marescaux, M. de Mathelin, and N. Padoy. Endonet: A deep
architecture for recognition tasks on laparoscopic videos. IEEE Transactions on Medical Imaging, 36(1):86–97,
2016.
[13] S. Ren, K. He, R. Girshick, and J. Sun. Faster R-CNN: Towards real-time object detection with region
proposal networks. In Advances in Neural Information Processing Systems, pages 91–99, 2015.
[14] Tool presence detection challenge results. http://camma.u-strasbg.fr/m2cai2016/index.php/
tool-presence-detection-challenge-results.
[15] K. Simonyan and A. Zisserman. Very deep convolutional networks for large-scale image recognition. arXiv
preprint arXiv:1409.1556, 2014.
5
�